
Plastic Surgery

UNLV Health Plastic Surgery’s group of talented physicians and caring support staff treat every patient with the highest respect, care and attentiveness. 
2025 Vegas Viewer’s Choice Awards
Gold: Augmentation, Liposuction, Plastic Surgeon
Silver: Reconstructive Surgery
Cosmetic Surgery
- Abdominoplasty
- Blepharoplasty
- Breast Augmentation
- Breast Reduction
- Dermabrasion
- Face Lift
- Fat Injection
- Laser Treatments
- Liposuction
- Rhinoplasty
- Thighplasty
Reconstructive Surgery
- Breast Reconstruction
- Cleft Lip and Palate Repair
- Craniofacial Surgery
- Diep Flap
- Scar Revision
- Skin Cancer Removal
- Skin Grafts
- Tissue Expansion
BREAST RECONSTRUCTION
Reconstructive breast surgery focuses on restoring the shape, appearance, and symmetry of the breast, usually after mastectomy, lumpectomy, or trauma. It can be performed immediately at the time of cancer surgery or delayed until after other treatments like chemotherapy or radiation.
Immediate vs Delayed
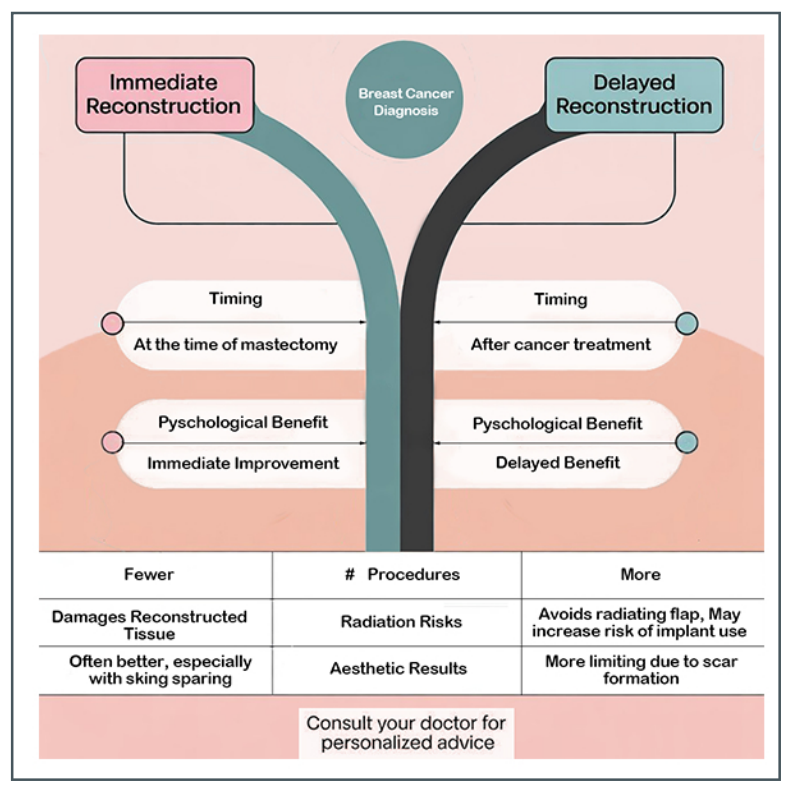
Immediate – Rationale
- Psychological benefit:
- Immediate restoration of breast contour helps reduce the emotional trauma of mastectomy
- Associated with better body image and self-esteem early in the recovery process
- Fewer surgeries:
- Combining mastectomy and reconstruction into one operation can minimize the number of anesthetic events and hospital stays
Immediate – Approach
- Often performed with skin-sparing or nipple-sparing mastectomy
- Options include:
- Implant-based reconstruction: Direct-to-implant or tissue expander-implant approach
- Autologous reconstruction: Using patient’s own tissue (e.g., DIEP flap)
- Requires close coordination between oncologic and reconstructive surgeons
- Suitability may depend on:
- Tumor size and location
- Need for adjuvant radiation therapy
- Patient preference and comorbidities
Delayed – Rationale
- Oncologic priorities first:
- Reconstruction is postponed to allow full focus on cancer treatment, including chemotherapy and radiation
- Avoids compromising reconstruction outcomes due to post-mastectomy radiation effects
- Better planning for complex cases:
- Allows time for patient to consider options and achieve medical optimization . Ideal when prognosis is uncertain or further surgery may be anticipated
- Radiation therapy impact:
- Radiation can negatively affect reconstructed tissues (particularly implants)
- Delaying reconstruction can avoid exposing the reconstruction site to radiation-induced fibrosis, contracture, or implant loss
Delayed – Approach
- Performed months to years after mastectomy, once cancer treatment is complete. Often used for autologous reconstruction, as tissues are more resilient to previous radiation damage
- Implant-based reconstruction is also possible, though outcomes may be compromised if radiation was administered
Implant-Based Reconstruction
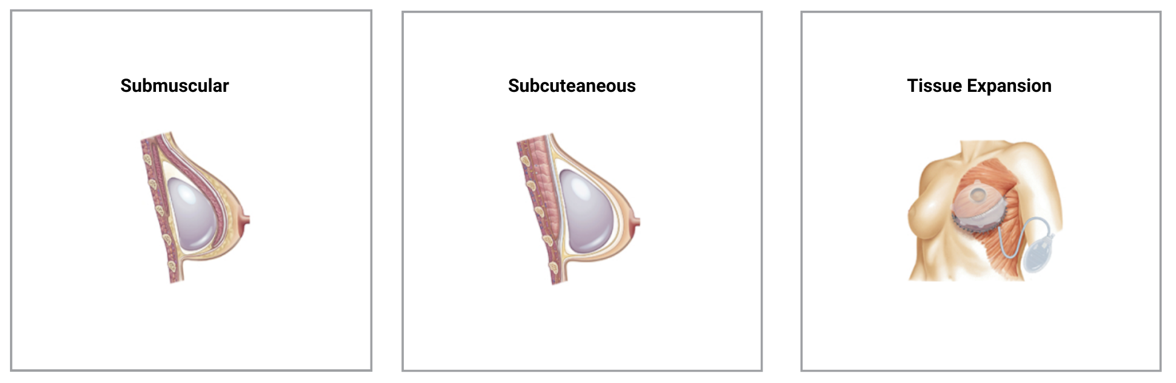
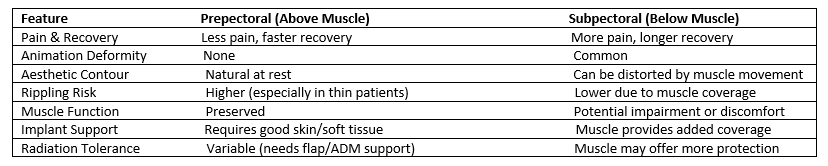
Placement of the implant: Below the muscle vs Above the muscle
Tissue Expander + Implant
- A temporary expander is placed to gradually stretch the skin and muscle
- Later replaced with a permanent silicone or saline implant
- Direct-to-Implant Reconstruction
- Implant placed immediately at the time of mastectomy (bypassing expander phase)
- Often requires supportive mesh (acellular dermal matrix like AlloDerm or synthetic mesh
Dermal Matrix
Is a surgical mesh used in breast reconstruction after a mastectomy to provide soft tissue coverage and support for breast implants. It is derived from human cadaver skin, and the cells are removed, leaving a supportive framework for the patient’s won tissue to integrate with. AlloDerm is often used in two-stage breast reconstruction, where it helps support the tissue expander during the initial stage and the permanent implant later on. It reinforces the soft tissue coverage over the implant and helping to prevent implant exposure or rippling. It may require extended use of drains.
Autologous Tissue/Flap
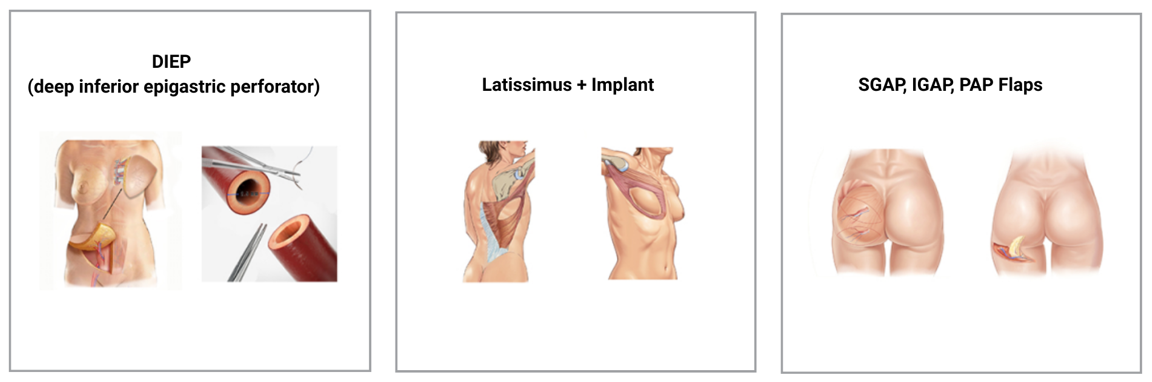
DIEP stands for Deep Inferior Epigastric Perforator flap. This method uses skin and fat from the lower abdomen (similar to a tummy tuck) to create a new breast.
How it works:
- The surgeon removes skin and fat-but not muscle-from the lower belly
- Tissue is carefully reconnected to blood vessels in the chest using microsurgery
- This tissue forms the new breast
Key feature: No abdominal muscle is taken, which helps preserve core strength and recover.
Latissimus Dorsi Muscle Flap
- This method uses muscle, skin, and fat from the upper back (latissimus dorsi muscle) and often combines it with a breast implant to reconstruct the breast
- How it works:
- A portion of the latissimus dorsi muscle along with some skin and fat is moved from the back to the chest.
- The tissue stays connected to its original blood supply (a “pedicled flap”)
- A breast implant is placed underneath to provide shape and volume
Key feature: Uses your own tissue but still requires an implant for desired fullness
AGAP/IGAP Flaps (Superior/Inferior Gluteal Artery Perforator)
- Tissue from the buttocks; used when abdominal tissue is unavailable
PAP Flap (Profunda Artery Perforator)
- Tissue from the upper inner thigh
Microsurgical free tissue transfer. These flaps are technically demanding and have shorter donor vessels on which to transfer the tissue. They may also be limited in volume. Used when abdominal tissue is unavailable due to prior surgery.
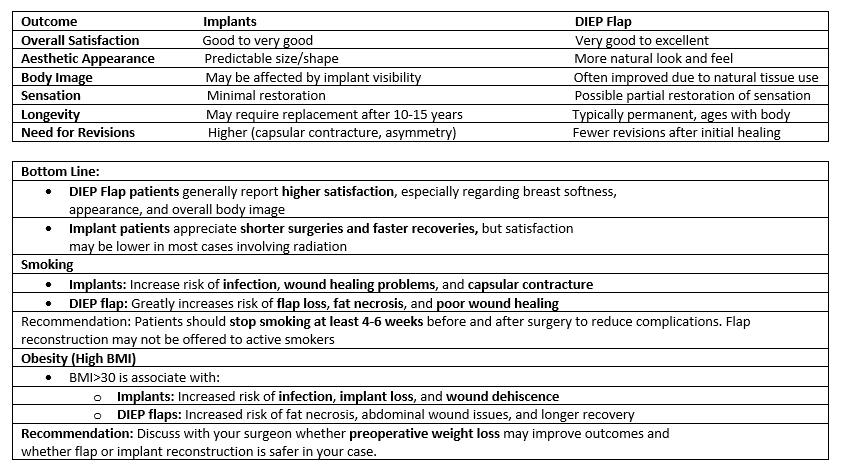
Comparison Of Two Techniques

Nipple & Areola Reconstruction
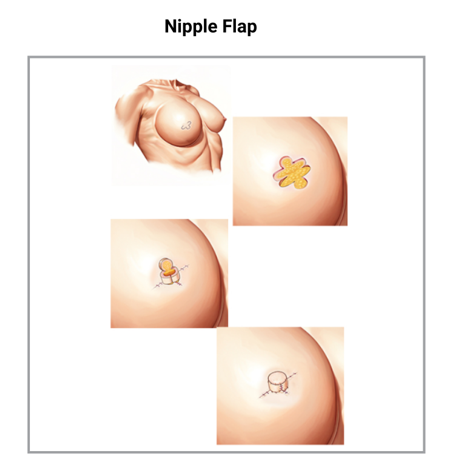
- Nipple-sparing Mastectomy: Preserves the patient’s natural nipple when oncologically safe
- Nipple Reconstruction: Using local skin flaps to create a projecting nipple
- Why areola tattoos are done: After breast reconstruction, the nipple-areola complex may be removed or altered. Areola tattoos can help recreate the look ad color of the areola, adding a realistic touch to the reconstructed breast
- Timing: It’s generally recommended to wait at least 3 months after the final breast reconstruction procedure before getting an areola tattoo to allow for adequate healing
- Procedure: The involves a tattoo artist or surgeon using pigments to create a realistic-looking areola on the reconstructed breast
- 3D effect: 3D tattooing can create a more lifelike appearance by using shading and depth to simulate the texture and contours of a natural areola
- Options: Some individuals may choose to have the nipple itself reconstructed surgically, while others may opt for a 3D nipple tattoo alone
- Benefits: Areola tattoos can improve body image, boost confidence, and reduce the feeling of being incomplete after breast reconstruction
Fat Grafting/Secondary Procedures
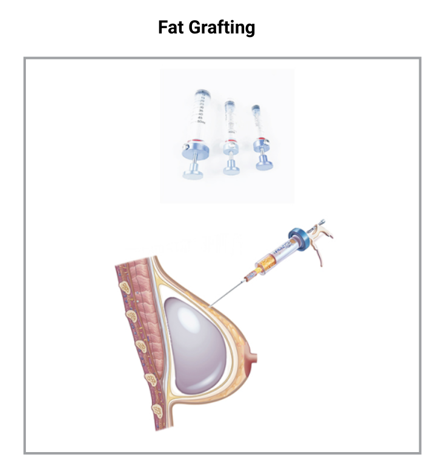
Fat Grafting (Lipofilling)
What it is: Fat is harvested from areas such as the abdomen, thighs, or flanks via liposuction, processed, and then injected into the breast to improve contour, correct volume deficiencies, and soften transitions around the reconstructed breast
Fat Graft “Take” Rate:
- On average, 50% to 70% of the transferred fat survives
- Because not all fat survives, multiple sessions (typically 1 to 3) are often required for optimal results
Benefits of Fat Grafting:
- Improves contour irregularities
- Softens implant edges
- Enhances skin quality-especially in radiated tissues
- Minimally invasive with short recover time

Grading (Baker Classification):
- Grade I: Breast is soft and appears natural
- Grade II: Breast is slightly firm but looks normal
- Grade III: Breast is firm and looks abnormal
- Grade IV: Breast is hard, painful, and clearly misshapen
Procedure to Correct Contracture:
- Capsulotomy: Surgical release of the capsule (less commonly performed)
- Capsulectomy: Complete removal of the capsule, often combined with implant replacement
- Conversion to Autologous Reconstruction: In cases of sever contracture, surgeons may recommend switching to tissue-based reconstruction (e.g., DIEP flap) for better long-term outcomes
- Fat Grafting Prior to Implant Replacement: May improve the radiated tissue bed and reduce recurrence risk
Craniofacial Surgery
- Cleft Lip & Palate
- Craniosynostosis
- Hemifacial Microsomia & Microtia
- Pierre Robin
- NV Craniofacial Team
- Facial Fractures
Craniofacial surgery is a specialized field of plastic surgery that deals with congenital and acquired deformities of the skull, face, and jaws. It encompasses a wide range of conditions affecting the bones, soft tissues, and sometimes the brain, eyes, ears, heart, or urogenital system.
CLEFT LIP PALATE
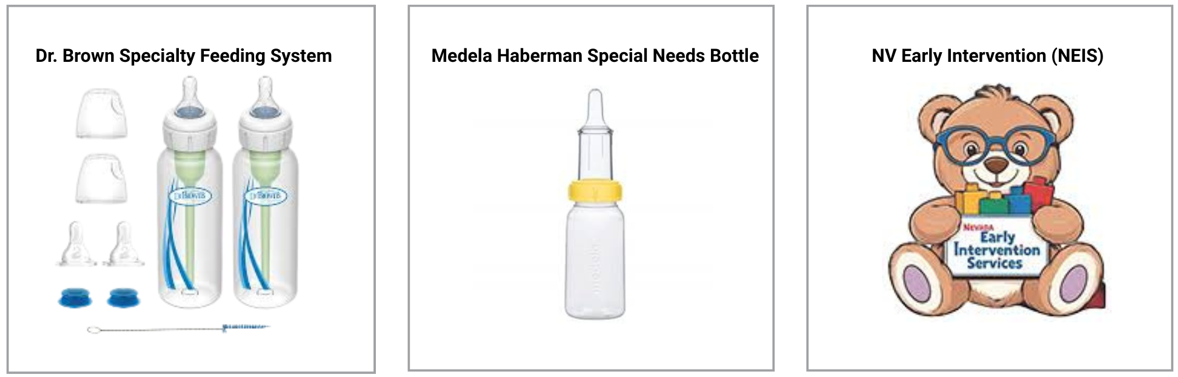
Feeding a Baby with a Cleft Palate – Babies with a cleft palate will not be able to breast feed and cannot use a regular baby bottle as they cannot generate enough suction due to the cleft. Babies with a cleft lip may also have trouble with forming a lip seal due to the separation in the lip muscle. These children need a special bottle.
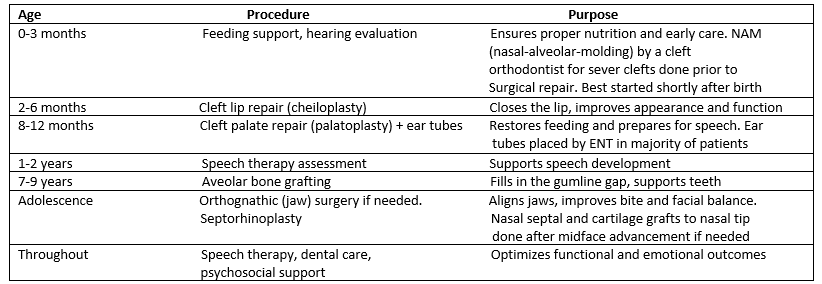
Stages of Cleft Reconstruction – Cleft lip repair is typically performed within the first 3 months of life with or without prior Nasal Aveolar Molding (NAM). Cleft palate repair is done at 8-12 months prior to the development of speech and language as well as coordinated with an ENT doctor for ear tubes placed at the time of surgery. Procedures are done at different ages to minimize potential negative effects of surgery on facial growth.
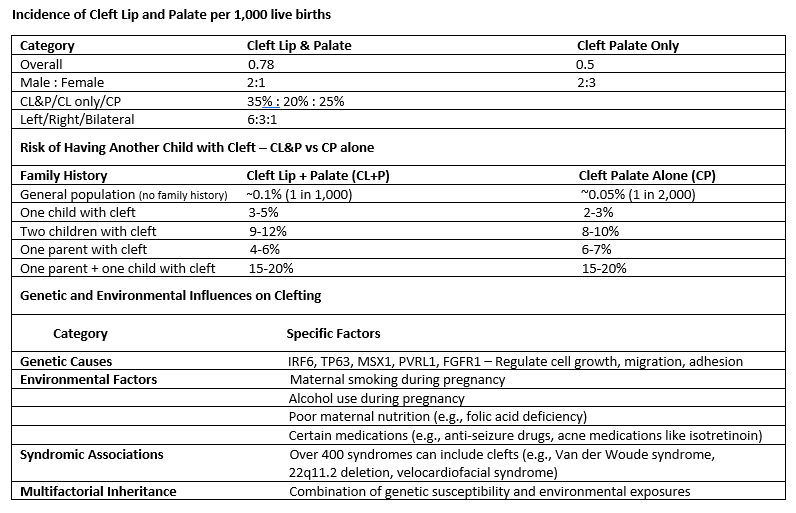
Cleft Incidence & Genetics – Cleft lip and cleft palate are among the most common congenital conditions affecting children worldwide. Approximately 1 in every 1000 babies is born with a cleft lip, cleft palate, or both. These conditions occur early in pregnancy when the tissues that form the lip and palate fail to fully come together.
FEEDING
Babies with a cleft palate cannot separate their mouth from their nose due to the cleft. This prevents the generation of a normal suction force and allows feeding material to enter the nose. Feeding requires a special bottle into which breast milk or other feeds can be transferred. Babies should be more upright when fed to use gravity as an assist.
- Positioning: Hold your baby in an upright position (at about a 45-degree angle) to help prevent mild from flowing into the nose
- Pacing: Watch for signs your baby needs a break (pausing, coughing, or milk leaking from the nose) and pace feedings to prevent choking
- Burping: Expect to burp your baby more frequently during feeds to help release swallowed air

The Nevada Early Intervention Services (NEIS) System provides services to children birth until three with developmental delay or disabilities, and their families. Feeding instructions are available. Speech evaluation and therapy for ages 1-3. (CCSD for Speech therapy ages 4 and older) This evaluation is free of charge.
NEIS 1161 S Valley View Blvd., Las Vegas, NV 89102 Phone: 702-486-7670
CLEFT INCIDENCE AND GENETICS
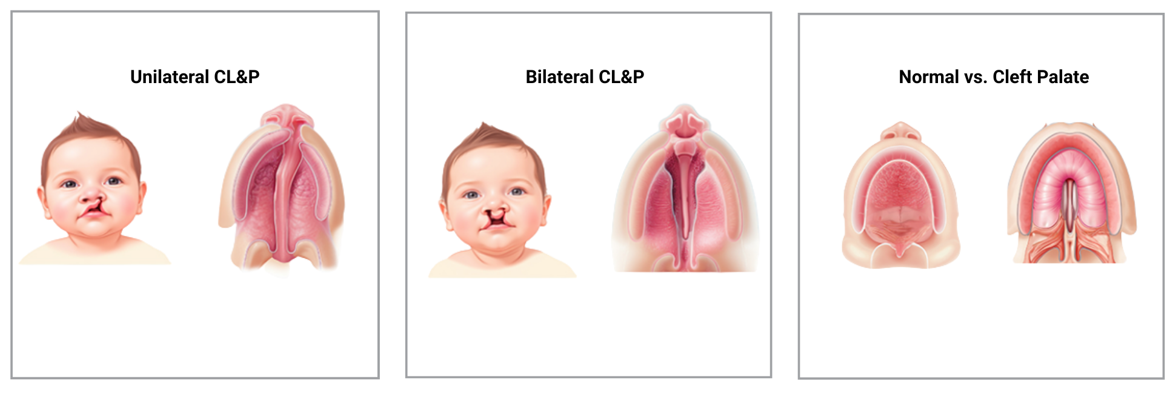
Types of Clefts:
- Cleft Lip (CL): An opening in the upper lip that can be unilateral (one side) or bi-lateral (both sides. It can range from a small notch to a large gap extending into the nose
- Cleft Palate (CP): An opening in the roof of the mouth, which can involve the soft palate (back) alone or extend to the hard palate (front)
- Cleft Lip and Palate (CLP): A combination of both, where both the lip and palate are affected
- Submucous Cleft Palate: A less visible form where the cleft is covered by the lining (mucosa) but the soft palate muscles are separated
This type of cleft is diagnosed by physical examination – there is a bifid or double uvula, a visible separation in the soft palate muscle seen as a shadow under the mucosa, and a midline V-shaped notch can be felt at the posterior edge of the hard palate. It is estimated that 20% will have speech issues requiring surgery but repair is deferred until speech can be assessed.
STAGES OF CLEFT RECONSTRUCTION
Why it is important to be seen soon after birth
- Nasal Alveolar Molding (NAM) is best performed early for the most severe clefts. It requires a dental impression, which is performed under general anesthesia, ideally in the first month of life
- Molding continues for approximately 3 months with the cleft orthodontist who can also help with staged palate repair (soft palate repair at 8 months, hard palate at 5 years) to minimize growth problems

Your child’s care plan will be personalized based on their unique needs and growth milestones.
Ages 12-17
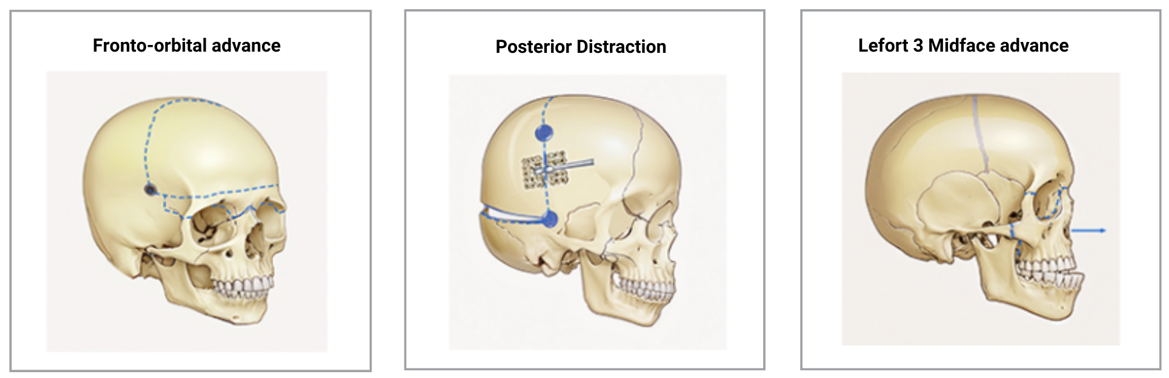
- Early repair of both the hard and soft palate result in a large percentage of patients needing Lefort 1 advancement due to the growth deficiency of the midface
- Final septorhinoplasty for cleft nasal deformity is done in this age group as nasal growth is complete. The septum is central for nasal growth and should not be addressed in early growth years. Cartilage grafts, important for creating a symmetric nasal tip, also do not grow, are placed at this age
Craniosynostosis
Craniosynostosis is a condition where one or more of the sutures (joints) in a baby’s skull close too early, before the brain has finished growing. This can affect the shape of the head, put pressure on the brain, and sometimes impact development.
Types Based on Sutures Involved:
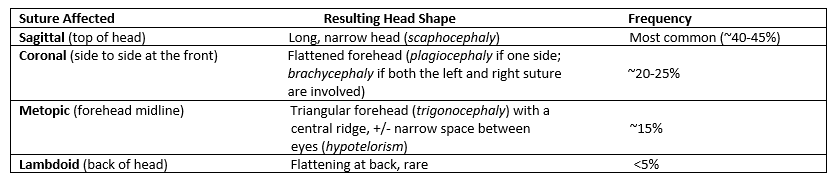
Syndromic vs. Non-Syndromic Craniosynostosis
Non-syndromic Forms

Non-Syndromic Craniosynostosis
This is the most common form and usually involves just one suture. It happens without other medical problems and typically occurs randomly.
Syndromic Craniosynostosis
Involves multiple sutures and is part of a genetic syndrome. These cases often include facial differences and other anomalies. Common syndromes include:
- Crouzon syndrome
- Apert syndrome
- Pfeiffer syndrome
- Saethre-Chotzen syndrome
- Muenke syndrome
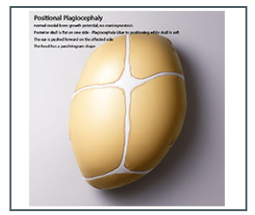
Positional Plagiocephaly
Molding Helmets vs. Craniosynostosis Surgery
It’s important to understand that molding helmets alone do not treat craniosynostosis. Helmets can help reshape the head in cases of positional plagiocephaly (flat head syndrome), which occurs when a baby lies in one position too much but has normal open sutures.

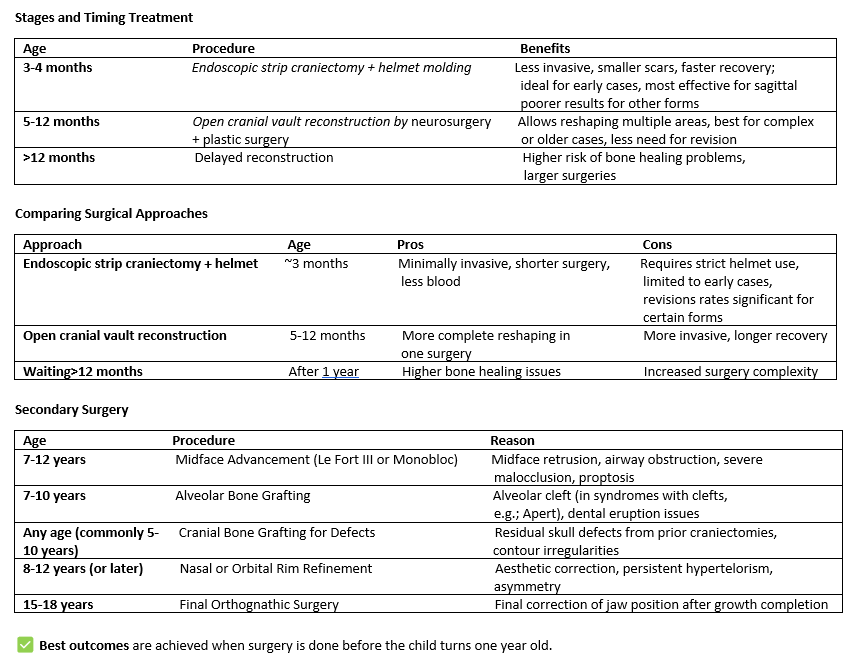
Treatment and Timing
Why Early Treatment Matters
Early reconstruction gives the brain room to grow when it is growing the fastest and helps normalize the skull shape while bones are still soft and flexible. Delaying surgery beyond 12 months can lead to larger bone gaps, longer surgeries, and higher rates of the need for secondary surgery
Associated Anomalies
Brain – Hydrocephalus (fluid buildup), Chiari malformation
Eyes – Vison problems due to pressure or orbital changes, or problems with lid closure due to shallow orbits in some syndromic forms
Airway – Breathing difficulties in syndromic cases where the orbits and midface have growth deficiencies
External Referrals – Our partnership with health professionals in the community is key to our success at UNLV Health. It is our goal to assist you with referring a patient to UNLV Health and ensure they receive the care they need. Referral team members are available to assist referring physicians by calling 702-671-5110.


